I touched on progesterone (P4) in my last transgender update post. I am not quite sure if progesterone is working in the way I want it to. My biggest annoyance with it is feeling like my brain is on fire just before trying to sleep.
Rewind to late February 2024, for almost three weeks my progesterone dose was doubled to 400 mg of oral, micronised, compounded progesterone – 200 mg twice a day. That’s up from the 200 mg once at night.
I had also ceased finasteride. And finasteride interferes with the progesterone (oral) pathway conversion to neurosteroids such as allopregnanolone. This is because finasteride blocks *most* of the activity (~70%) of the 5-alpha reductase (5AR) enzyme. In turn, reducing levels of allopregnanolone – or at least slowing their conversion to neurosteroids.

My sleep quality has been pretty broken for a while now. Look at those orange blocks. And here I was looking forward to some of the benefits from progesterone. Anxiolytic? Yes please! Sleep improving? Definitely!

Instead I get this whole brain fire thing and feel like I’ve taken an anxiogenic. That got me thinking, brain on fire? Throw in some formication and it’s what feels like a glutamate rebound or surge. Excitotoxicity perhaps?
I’ve experienced similar feelings while withdrawing from pregabalin (decreases glutamate levels) and trusty old diazepam (increases GABA levels). Definitely that same feeling though. It appears that taking what I would consider a small dose (2 mg) of diazepam negates the insomnia pretty well. Even though diazepam isn’t a terribly good choice for sleep. It takes me from being a wired insomniac to sleeping beauty in about an hour.
Another interesting side effect I am seeing a lot more of is dissociation. Ordinarily, I would only experience this while in high stress, high anxiety situations but recently I’m noting it a lot more just doing chores around the house – which is a little concerning.
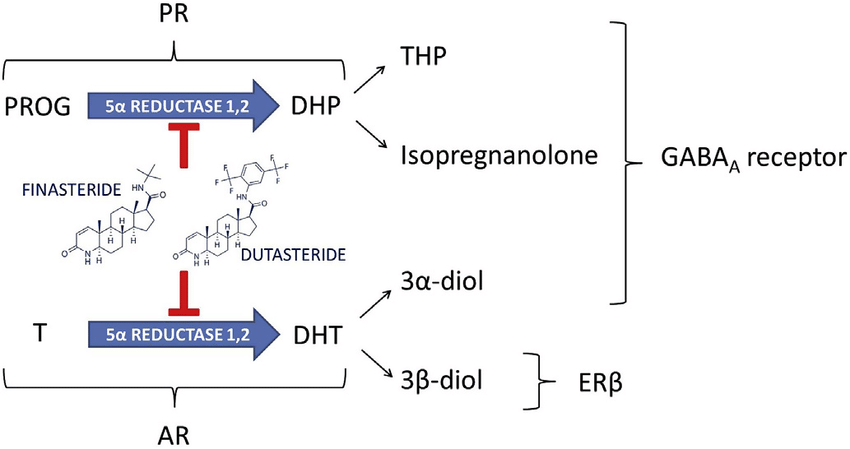
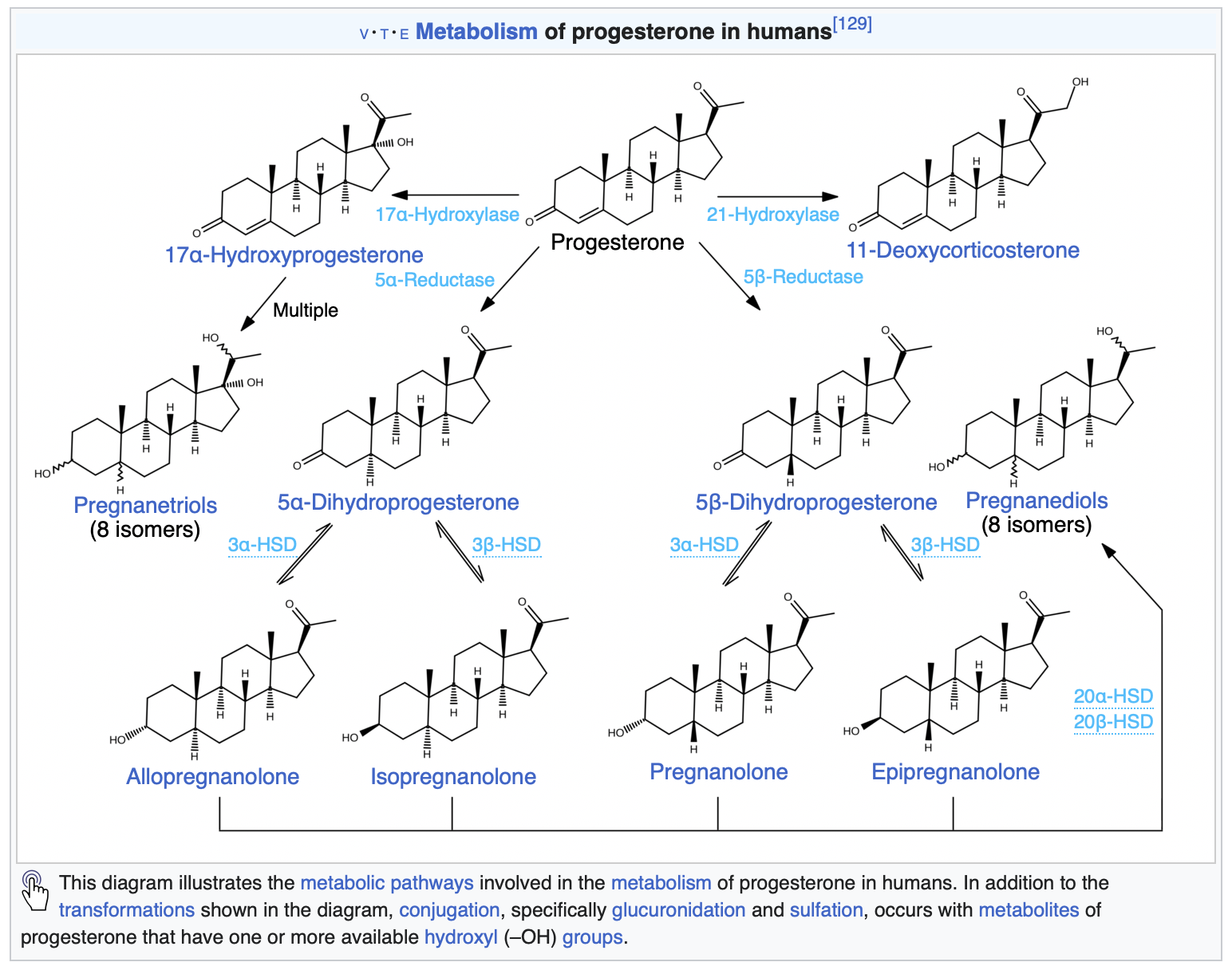
Regardless, it seems that something is messing with my GABAergic system and metabolites of progesterone fit the bill. Armed with my two-thirds of a biomedical science degree I went digging for more information on the metabolites. Up above is an image from my last health blog post. Note the action of finasteride on progesterone – blocking allopregnanolone (THP) and isopregnanolone.
I wonder if moving to a more potent 5AR blocker, such as dutasteride, would reduce the side effects of a higher dose of progesterone? A question for my endocrinologist I suppose. I restarted my finasteride to at least partially block some of the following progesterone metabolites. Let’s look at the metabolites a little closer and how they act.
Allopregnanolone (Tetrahydroprogesterone or THP)
Positive allosteric modulator
9 hours
Pregnanolone
Positive allosteric modulator
1 – 3.5 hours
Isopregnanolone
Negative allosteric modulator
14 hours
Targets allopregnanolone only
Epipregnanolone
Negative allosteric modulator
Half-life unknown
Alright, so a bunch of neurosteroids are doing a bunch of things. A few are being blocked, but also produce negative side effects when they weren’t blocked. Hormones are messy. Where does that leave me? I guess I am left questioning whether I should be taking progesterone at all. At minimum a dose reduction is definitely called for. I will probably return back to 200 mg and see what symptoms, if any, follow.
My search revealed some interesting data with overlap in symptoms shared with premenstrual syndrome (PMS) and premenstrual dysphoric disorder (PMDD) in cisgender women.
PMDD is believed to be caused by fluctuations in gonadal sex hormones or variations in sensitivity to sex hormones.
If sensitivity to level shifts is reason for the negative side effects, then single or even twice daily doses are probably not enough to smooth out the levels of neurosteroids for me, allowing me enter a withdrawal state, perhaps? Brain on fire? This paper offers some great insight into the mechanisms behind it all with some interesting side notes on SSRIs.
Interestingly, SSRIs increase allopregnanolone levels in the brain, rapidly and at low doses, as demonstrated in rodents as well as in patients with depression.
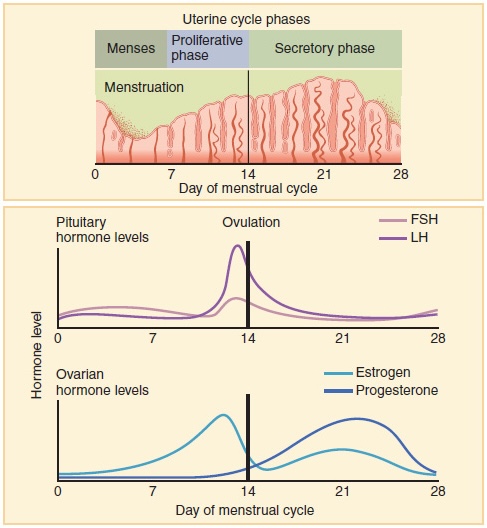
Could this be one of the reasons why I can’t tolerate SSRI/SNRIs? At the very least, it’s some food for thought. Worth noting that the original study has been questioned a little further along in the paper. Let’s circle back to those progesterone levels again. From Wikipedia
Progesterone levels tend to be less than 2 ng/mL prior to ovulation and greater than 5 ng/mL after ovulation.
What were my most recent levels again? 9.1 nmol/L or should I say 2.6 ng/mL (freedom units). That’s at 200 mg once daily at night, measured in the trough. I really need to ask myself, do I want to have symptoms of PMS/PMDD? Is that even a question that needs to be asked?
Looking at the levels on Table 1 in this paper give an idea where my levels line up. If you factor in the short half-life of most of the metabolites, once daily dosing is probably a bad idea. Ideally, I should look into getting the dose split to 100 mg twice daily.
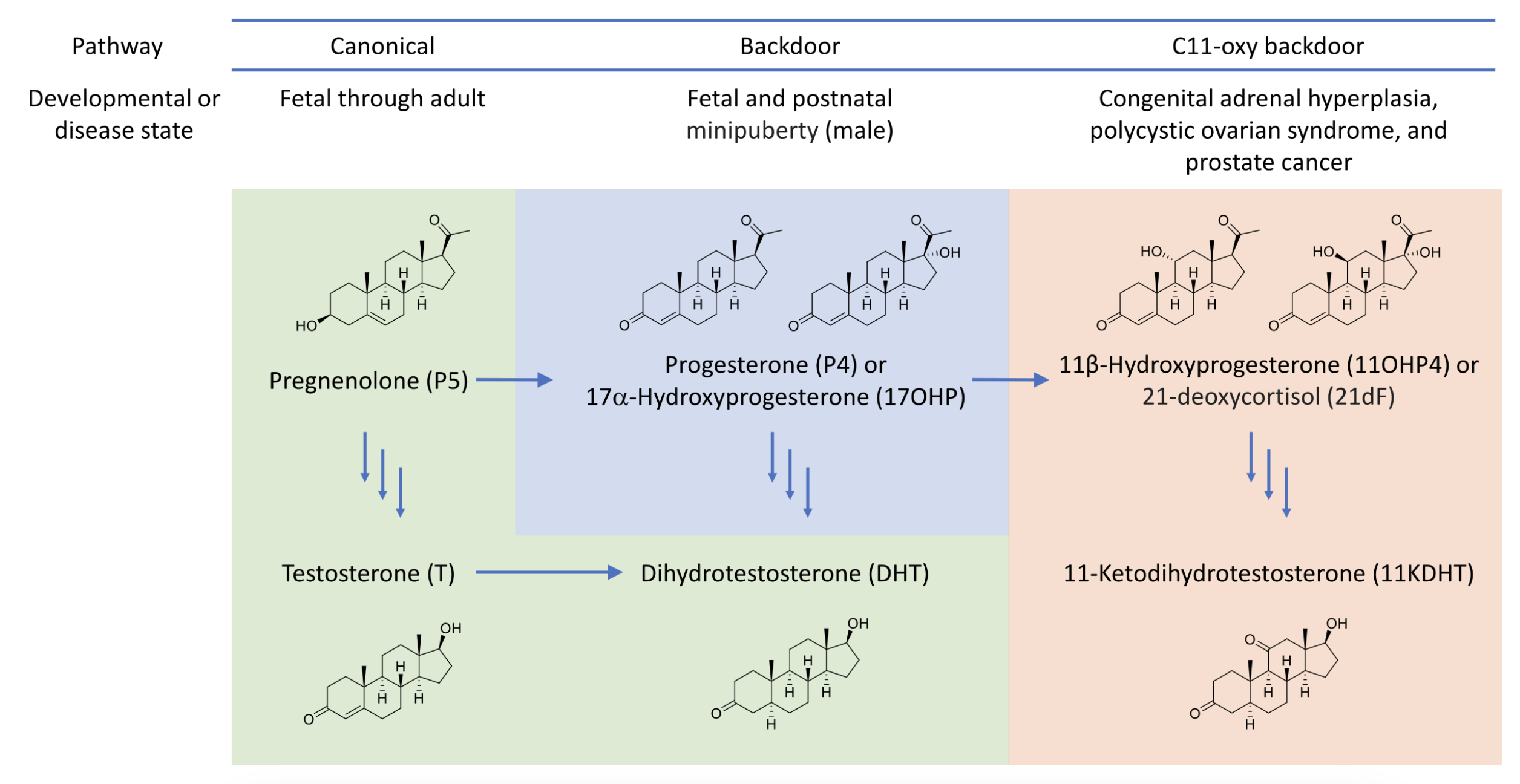
Of course I have to be mindful of negative risk such as the androgen backdoor pathway. This has the potential to generate unwanted androgens like DHT – which will affect the hair on my head. That’s why the finasteride is here to stay until most means of testosterone generation is removed from my system…
It’s not all bad though. Finasteride competes with progesterone for the 5AR enzyme – which results in even less 5AR being available for testosterone -> DHT conversion. Another point worth considering is that progesterone has a positive effect on bone-building cells (osteoblasts). This can help with avoiding or reducing effects of osteoporosis.
Touching on side effects I’ve noticed, Progesterone should increase libido. Which is something I do not want due to past trauma. However, I wonder if the finasteride side effects are at play here. Again, I don’t consider them negative side effects either.
Other oddities I’ve also noticed my facial hair has become darker at the higher progesterone dosing at 400 mg. My upper lip now has dark black hairs, that’s new and unwanted. It might be useful for IPL treatment. But now there’s shadow on my upper lip I never had before. It isn’t just the thinning of skin either. The hairs are black instead of blonde.
![]()
One big uncertainty is that I’m not sure what my levels of estradiol will be at the next blood test. Are the 200 mg of pellets doing their job properly? Or did they fail? Does the dose need to be increased?
For now, I’ve been supplementing the implant with the remainder of my 2 mg estradiol pills while the pellets stabilise. One pill gives me ~85 pmol/L in estradiol levels. I’ve only just ran out of those so now I’m adding in some of the estradiol gel (Sandrena branded). These gave ~200 pmol/L estradiol per dose according to my most recent blood tests. In theory with one a day, I should be guaranteed to be in the late follicular phase – regardless of the implant levels.
Anyway, that was one heck of an info dump. I think that sums everything up that has been on my mind lately.
TL;DR
400 mg oral progesterone makes my brain go on fire. Progesterone metabolite levels shifting around are very activating for me. I will now target cisgender progesterone levels in the late follicular phase. Hormones are complicated. One size fits most seems to be at play when it comes to progesterone. Nothing like some trial and error! 🙃